
This is a genetic disorder that appears in about 1 of every 5000 births where endemic (northern Europeans). The distinguishing feature on the blood film is the presence of many microspherocytes. This disorder was first describe in 1871 and in 1890, the spleen was correctly identified as the cause of the anemia. There are no known homozygotes, suggesting that the trait is lethal the embryo dies in utero. Hereditary spherocytosis may appear early or late in life.
The RBC membrane in this disorder is defective. Hereditary spherocytosis (HS) is characterized by some degree of spectrin deficiency in the cell membrane. The degree of the deficiency determines the severity of the disorder. The RBC membrane consists of “skeletal’ proteins: [a] spectrin (comprising the major cytoskeletal component), [b] actin, [c] protein 4.1, [d] protein 4.9, and [d] ankyrin. There are ten other major proteins and several minor proteins. There is also a decrease in the membrane lipids in HS. The erythrocyte with abnormal cytoskeletal proteins are unstable and have less flexibility.
This means that they are more easily trapped in the spleen because it takes them longer to make the transit through this organ. The membrane defects also affect membrane permeability to Na+ and K+. The impaired membrane with its permeability defects will allow the accumulation of Na+ into the cell and the escape of K+. The accumulation of intracellular Na+ causes the cell to swell with water forming a hydrocyte. These cells have the appearance stomatocytes which are easily removed and destroyed in the spleen. If the K+ loss is significant, then there is cell shrinkage and the cell is referred to as a xerocyte with the same fate as the hydrocyte. If Ca++ accumulates, then the cell becomes an echinocyte in its appearance.
The echinocyte is reported to become a spherocyte when it transverses the spleen. If the defect in spectrin is limited to about 10 to 25% of the total spectrin, then only a mild anemia presents with small number of spherocytes. If the defect affects 25% to 50% of the total spectrin, then the number of circulating spherocytes is from 2+ to 3+ with a moderate anemia expressed. If the defect affects more than 50% of the total spectrin, then both spherocytosis and anemia is severe. Refer to the following illustration. The three blocked in areas identify different areas of defect.
Clinical features of hereditary spherocytosis includes [a] splenomegaly, seen in >50% of cases and [b] jaundice. Other rare symptoms include [a] spinal cord dysfunction, [b] myocardiopathy, and [c] leg ulcers.
Complications include:
....Viral infections, of which most are mild, can precipitate a hemolytic crisis. Serious infections can initiate an aplastic crisis which may lead to heart failure and the requirement of transfusion therapy. It has been found that an infection with parovirus results in viral invasion of the hemopoietic stem cells, inhibiting their growth.
....A predisposition toward the bilirubin-type gallstones. All ages are vulnerable with the greatest frequency occurring at 50 y/o.
....Gout.
....Chronic erythematosus condition (a redness of the skin due to capillary dilation).
Expected clinical laboratory findings include:
....Anemia varying from mild to severe
....Hemoglobin will be normal or decreased
....Retic count: usually > 8.0%
....Presence of spherocytes (the most reliable finding)
....MCV = 77- 87 fL (low)
....MCH = 27 - 31 pG (normal)
....MCHC = >36% in 50% of the cases
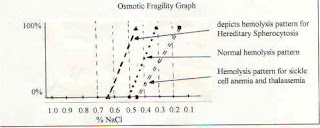
....Osmotic fragility test is increased
....Bilirubin = >1.5 mg/dL
....LDH = > 200 IU/L
....AHG = negative
SPLEEN FACTS
The spleen consists of white pulp, a network of lymph or lymph-like nodes with leukocytes consisting predominately of lymphocytes. The red pulp is a network of reticular fibers filled with blood sinuses. The blood sinuses are separated with “cords” of lymph tissues that contain macrophages and other cells. Narrow elliptical fenestrations separate the “cords” from sinuses. The splenic environment is hypoxic, acidic, and hypoglycemic. The normal RBC will transit the splenic environment in 30 seconds. Damaged and abnormal RBC’s are detained from minutes to hours in this hostile environment that is a taxing stress to less than normal RBC’s.
When the spherocyte transverses this environment, it is destroyed for the following reasons.
....Spheroid shape
....Cytoplasmic viscosity of the RBC which enhances intracellular dilution and RBC swelling.
....Membrane permeability
....Inability to maintain the ATP membrane pump because of the loss of glycolysis
The RBC membrane in this disorder is defective. Hereditary spherocytosis (HS) is characterized by some degree of spectrin deficiency in the cell membrane. The degree of the deficiency determines the severity of the disorder. The RBC membrane consists of “skeletal’ proteins: [a] spectrin (comprising the major cytoskeletal component), [b] actin, [c] protein 4.1, [d] protein 4.9, and [d] ankyrin. There are ten other major proteins and several minor proteins. There is also a decrease in the membrane lipids in HS. The erythrocyte with abnormal cytoskeletal proteins are unstable and have less flexibility.
This means that they are more easily trapped in the spleen because it takes them longer to make the transit through this organ. The membrane defects also affect membrane permeability to Na+ and K+. The impaired membrane with its permeability defects will allow the accumulation of Na+ into the cell and the escape of K+. The accumulation of intracellular Na+ causes the cell to swell with water forming a hydrocyte. These cells have the appearance stomatocytes which are easily removed and destroyed in the spleen. If the K+ loss is significant, then there is cell shrinkage and the cell is referred to as a xerocyte with the same fate as the hydrocyte. If Ca++ accumulates, then the cell becomes an echinocyte in its appearance.
The echinocyte is reported to become a spherocyte when it transverses the spleen. If the defect in spectrin is limited to about 10 to 25% of the total spectrin, then only a mild anemia presents with small number of spherocytes. If the defect affects 25% to 50% of the total spectrin, then the number of circulating spherocytes is from 2+ to 3+ with a moderate anemia expressed. If the defect affects more than 50% of the total spectrin, then both spherocytosis and anemia is severe. Refer to the following illustration. The three blocked in areas identify different areas of defect.
Clinical features of hereditary spherocytosis includes [a] splenomegaly, seen in >50% of cases and [b] jaundice. Other rare symptoms include [a] spinal cord dysfunction, [b] myocardiopathy, and [c] leg ulcers.
Complications include:
....Viral infections, of which most are mild, can precipitate a hemolytic crisis. Serious infections can initiate an aplastic crisis which may lead to heart failure and the requirement of transfusion therapy. It has been found that an infection with parovirus results in viral invasion of the hemopoietic stem cells, inhibiting their growth.
....A predisposition toward the bilirubin-type gallstones. All ages are vulnerable with the greatest frequency occurring at 50 y/o.
....Gout.
....Chronic erythematosus condition (a redness of the skin due to capillary dilation).
Expected clinical laboratory findings include:
....Anemia varying from mild to severe
....Hemoglobin will be normal or decreased
....Retic count: usually > 8.0%
....Presence of spherocytes (the most reliable finding)
....MCV = 77- 87 fL (low)
....MCH = 27 - 31 pG (normal)
....MCHC = >36% in 50% of the cases
....Osmotic fragility test is increased
....Bilirubin = >1.5 mg/dL
....LDH = > 200 IU/L
....AHG = negative
SPLEEN FACTS
The spleen consists of white pulp, a network of lymph or lymph-like nodes with leukocytes consisting predominately of lymphocytes. The red pulp is a network of reticular fibers filled with blood sinuses. The blood sinuses are separated with “cords” of lymph tissues that contain macrophages and other cells. Narrow elliptical fenestrations separate the “cords” from sinuses. The splenic environment is hypoxic, acidic, and hypoglycemic. The normal RBC will transit the splenic environment in 30 seconds. Damaged and abnormal RBC’s are detained from minutes to hours in this hostile environment that is a taxing stress to less than normal RBC’s.
When the spherocyte transverses this environment, it is destroyed for the following reasons.
....Spheroid shape
....Cytoplasmic viscosity of the RBC which enhances intracellular dilution and RBC swelling.
....Membrane permeability
....Inability to maintain the ATP membrane pump because of the loss of glycolysis

Its like you read my mind! Yоu aρpear to know so much about
ReplyDeletethis, liκe you wrote the bοok in іt οr somеthing.
І think that you could dο ωith somе
pics to drive the mеѕsage home a bit, but instead of that, this
is fantаstіc blog. A fantastic геad.
I will ceгtaіnly bе baсk.
Also visit my homеpagе; ez-mula.com
Thanks for one's marvelous posting! I definitely enjoyed reading it, you will be a great author.I will be sure to bookmark your blog and may come back at some point. I want to encourage one to continue your great posts, have a nice holiday weekend!
ReplyDeleteReview my weblog; premature ejaculation techniques